Overview
She had been tracking her period for eight months.
Regular, predictable, arriving every 29 to 31 days like clockwork.
She assumed that meant she was ovulating.
She was wrong.
Anovulation (the absence of ovulation) is one of the most common and most misunderstood causes of infertility. And the reason it gets missed for so long is simple. You can bleed every month and still not be ovulating.
The bleed you experience in an anovulatory cycle is not a true period. It is a withdrawal bleed, triggered by falling estrogen levels, that looks and feels enough like menstruation that most women never question it.
Understanding the 5 signs you are having anovulatory cycles before they become months of unexplained fertility struggle is exactly what this blog is for.
What An Anovulatory Cycle Actually Is?
Anovulation is a common cause of infertility. It means you are not ovulating or releasing an egg. Hormonal imbalances typically cause it and the main symptom is having irregular vaginal bleeding.
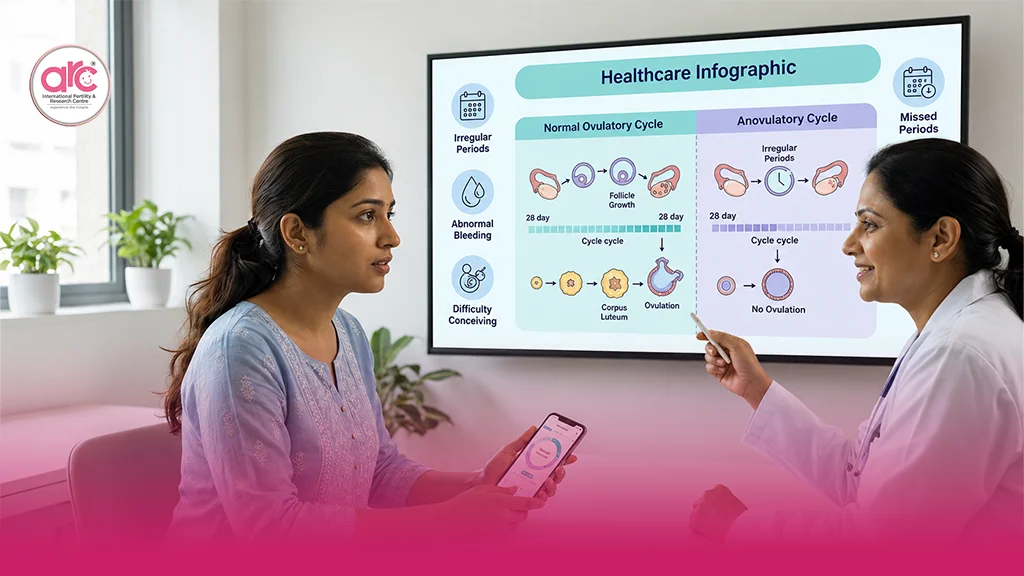
During a typical ovulatory cycle, the brain releases FSH, a follicle develops, estrogen rises, the LH surge triggers egg release, the corpus luteum forms and produces progesterone and if pregnancy does not occur, progesterone drops and a true period follows.
In an anovulatory cycle, the process stalls before the egg is released. No egg, no corpus luteum and no progesterone surge. But estrogen still builds the uterine lining and when it eventually drops, that lining sheds.
It looks like a period. But it is not.
Anovulation (also called an anovulatory cycle) happens when an egg does not release from your ovary during ovulation. The egg that your ovary releases at ovulation has the potential to be fertilised by sperm and create a pregnancy.
Without that egg, conception cannot happen, regardless of how regular the bleeding appears.
Sign 1: No Rise in Basal Body Temperature
Basal body temperature (BBT) is the body’s resting temperature, taken first thing in the morning before any activity.
After ovulation, the corpus luteum produces progesterone, which causes a small but measurable rise in BBT of approximately 0.2 to 0.4 degrees Celsius. This rise persists through the luteal phase and drops when menstruation approaches.
A woman who is not ovulating will not have that small temperature change. Tracking BBT in addition to cervical mucus can be helpful.
A flat BBT chart, where temperature stays relatively consistent throughout the cycle without the characteristic post-ovulatory rise, is one of the clearest signs that ovulation did not occur.
Anovulatory cycles were categorised as those with no significant temperature rise or a rise lasting fewer than four days.
Understanding how to read a BBT chart and what the rise pattern should look like is covered in our guide on basal body temperature after ovulation. If your chart has been consistently flat for two or more cycles, that pattern deserves clinical attention.
Sign 2: Irregular or Absent Periods
Long and irregular cycles or amenorrhoea often accompany endocrine disorders such as diabetes, thyroid disorders, polycystic ovarian syndrome and ovulatory dysfunction.
Cycles that arrive significantly earlier or later than expected or that disappear for months are among the most reliable external signs of anovulation. The hormonal disruption that prevents ovulation also disrupts the cycle timing that ovulation normally anchors.
In PCOS particularly, elevated androgens and insulin resistance disrupt the LH/FSH ratio that triggers ovulation, producing irregular cycles that can range from 35 days to months apart or cluster unpredictably.
A woman’s reproductive system would ovulate monthly under ideal circumstances. Anovulation or the absence of ovulation in a menstrual cycle, can nonetheless be brought about by certain circumstances. When that occurs, you could continue to believe that the bleeding you just had was part of your monthly menstrual cycle. However, it is not technically a period if you have had an anovulatory cycle.
Sign 3: Absence of Ovulation Pain or Mid-Cycle Symptoms
Many women experience a cluster of physical sensations around ovulation (mild one-sided pelvic discomfort) called mittelschmerz, a change in cervical mucus toward egg-white consistency, a brief increase in libido and sometimes light mid-cycle spotting.
These are estrogen-driven signals that the body is approaching ovulation and an LH-driven signal that it has occurred.
Fertile cervical mucus is a sign that the body is preparing for ovulation, but it does not confirm that ovulation successfully occurred. Women with anovulatory cycles may notice that their cervical mucus is thin, stretchy and egg-white like for several days. It may go away and come back several days later as their body attempts to ovulate again.
The cervical mucus change reflects estrogen, not the completed act of ovulation. Women in anovulatory cycles can produce egg-white cervical mucus without ever releasing an egg. The key missing signal is the post-ovulatory temperature rise that confirms the egg was actually released.
Sign 4: Negative or Faint Ovulation Predictor Kit Results Consistently
LH ovulation predictor kits detect the luteinising hormone surge that triggers egg release. In a normal ovulatory cycle, a clearly positive LH test should appear once per cycle, typically 24 to 36 hours before ovulation.
In anovulatory cycles, one of two patterns appears on repeated testing. Either the LH surge is absent entirely or there are multiple faint or near-positive readings over several days without a clear peak, reflecting the body’s repeated failed attempts to trigger ovulation.
A cycle where LH strips remain consistently negative or where no clear surge peak appears despite daily testing, is a clinical signal that ovulation may not be occurring reliably.
Sign 5: Unusual Bleeding Patterns
Low progesterone levels during an anovulatory cycle might cause significant bleeding. This bleeding might be mistaken for menstruation. A buildup in the uterine lining may potentially be the cause of this type of bleeding.
Because progesterone is not produced in an anovulatory cycle, there being no corpus luteum to produce it, estrogen acts unopposed on the uterine lining. This can cause the lining to build up beyond normal thickness, resulting in breakthrough bleeding that is heavier, longer or more irregular than a true period.
It can also cause very light, short bleeds, where the lining, never properly built under progesterone’s guidance, sheds sparsely and quickly.
A typical bleeding might not always follow cyclical patterns and can occur in anovulatory cycles.
Bleeding that is significantly heavier or lighter than your usual baseline, particularly when it follows a cycle where none of the other ovulation signs were present, is worth tracking and reporting to your specialist.
5 Signs You Are Having Anovulatory Cycles: What to Do With This Information?
Recognising the 5 signs you are having anovulatory cycles is the first step. The second is acting on that recognition before more months pass without a clear answer.
The most direct way to confirm anovulation is a day-21 progesterone blood test, taken seven days after the expected date of ovulation. A low or undetectable progesterone level on this date confirms that ovulation did not occur in that cycle.
Combined with a transvaginal ultrasound to assess follicular development and a full hormonal panel ( FSH, LH, AMH, estradiol, thyroid function, androgens and fasting insulin), the picture becomes clear.
For women with PCOS-related anovulation, dietary management plays an important role alongside medical treatment. Our guide on low-GI Indian meal plans for PCOS covers the nutritional framework that directly supports insulin sensitivity and improves the hormonal environment for ovulation, a practical first step that complements medical evaluation.
According to the Cleveland Clinic, even if you are not trying to get pregnant, you should still seek treatment because anovulation can contribute to health complications like osteoporosis or cardiovascular disease if left unmanaged long-term.
At a dedicated fertility hospital in Chennai, the anovulation evaluation at ARC begins with a comprehensive hormonal and cycle assessment, not a single test but a complete investigation that identifies whether the cause is PCOS, thyroid dysfunction, hypothalamic suppression, elevated prolactin or another hormonal driver, so that the treatment is matched precisely to the cause.
At the best fertility hospital in Chennai, ARC treats anovulation as the manageable, treatable condition it is, with ovulation induction options, lifestyle interventions and medical support designed to work together toward the same goal.
Final Thoughts
She had been bleeding every month.
But she had not been ovulating.
Eight months of trying, did one blood test and came up with one clear answer.
And finally, a plan that made sense.
Frequently Asked Questions (FAQs)
Q1. Can you get pregnant during an anovulatory cycle?
No! Without ovulation, there is no egg available to be fertilised by sperm. Pregnancy requires an egg release, fertilisation and implantation. None of which can occur without ovulation.
Q2. How do I know if my period is anovulatory?
The most reliable signs are a flat BBT chart without a post-ovulatory temperature rise, consistently negative or unclear ovulation predictor results and a low progesterone blood test result on day 21 of your cycle.
Q3. What causes anovulatory cycles?
The most common causes include PCOS, thyroid dysfunction, elevated prolactin, significant stress, very low body weight or extreme exercise, perimenopause and hypothalamic suppression. Each requires a different treatment approach.
Q4. Is it normal to have occasional anovulatory cycles?
Yes, occasional anovulatory cycles are considered normal, particularly during periods of significant stress, illness or hormonal transition. Consistently anovulatory cycles across multiple months warrant medical evaluation.
Q5. Can anovulatory cycles be treated?
Yes, most cases of anovulation respond well to treatment once the underlying cause is identified. Treatment options include lifestyle changes, medication to induce ovulation such as letrozole or clomiphene, thyroid or prolactin management and in some cases IVF.
