Overview
You’ve been tracking your cycles religiously. The ovulation strips, the basal body temperature charts, the timed intimacy—everything by the book. Yet month after month, nothing. Your periods might be irregular or absent altogether. Perhaps you’ve noticed your libido isn’t what it used to be. And here’s the strange part: you’re not even breastfeeding, but you’ve got this odd milky discharge.
Welcome to the confusing world of hyperprolactinemia—a condition where a tiny pea-sized gland in your brain decides to wreak havoc on your fertility plans.
What Exactly Is Prolactin Anyway?
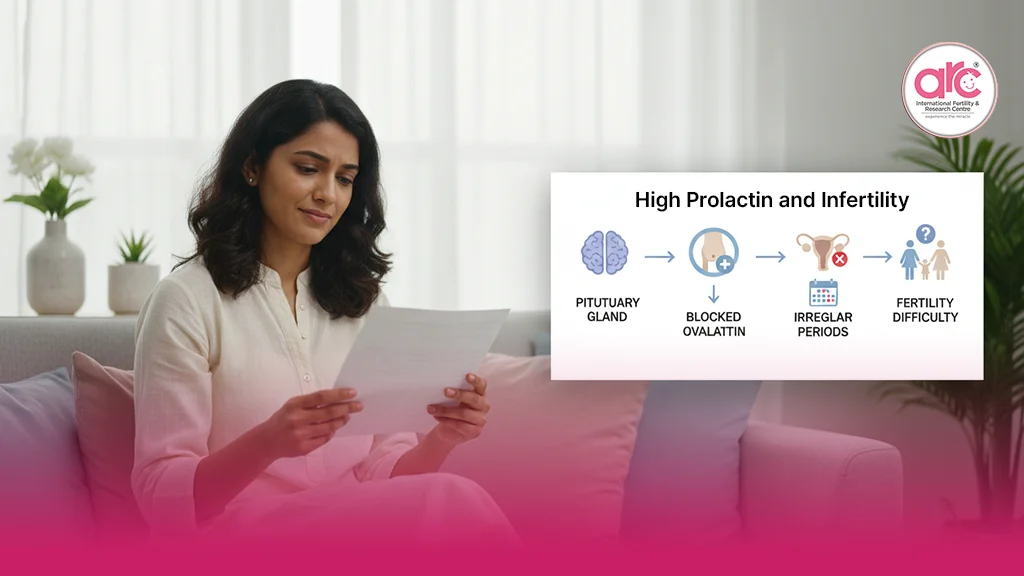
Think of prolactin as your body’s designated milk producer. It’s a hormone secreted by the pituitary gland, sitting snugly at the base of your brain. In the natural order of things, prolactin levels shoot up during pregnancy and after childbirth to stimulate breast milk production. It’s brilliant design, really—nature’s way of ensuring newborns get fed.
But prolactin doesn’t work in isolation. It’s part of an intricate hormonal conversation involving your hypothalamus, pituitary gland, and reproductive organs. When prolactin levels stay elevated outside of pregnancy and breastfeeding, this conversation gets scrambled. The result? Your reproductive system essentially hits the pause button.
The Domino Effect: How High Prolactin Sabotages Fertility
Here’s where things get interesting—and frustrating for anyone trying to conceive.
In women, elevated prolactin directly interferes with GnRH (gonadotropin-releasing hormone), the master regulator that kickstarts your reproductive cycle. When GnRH gets suppressed, it creates a cascade of problems:
- FSH and LH take a nosedive. These are the hormones responsible for maturing your eggs and triggering ovulation. Without adequate levels, your ovaries basically go dormant.
- Estrogen production drops. Lower estrogen means your uterine lining may not develop properly, even if by some chance you do ovulate.
- Your cycles become erratic or disappear entirely. Some women experience oligomenorrhea (infrequent periods), while others develop full-blown amenorrhea (no periods at all).
It’s like your body thinks you’re already pregnant or nursing, so why bother with another pregnancy?
In men, the story isn’t much better. Elevated prolactin suppresses testosterone production, and testosterone is the cornerstone of male fertility. The consequences include:
- Reduced sperm count and motility. Your swimmers aren’t just fewer in number; they’re also less capable of reaching their destination.
- Erectile dysfunction. High prolactin can dampen sexual desire and interfere with achieving or maintaining erections.
- Low libido. When your testosterone tanks, so does your interest in sex—which obviously doesn’t help the baby-making equation.
Men often dismiss these symptoms or attribute them to stress or aging. But if you’re experiencing these issues alongside infertility, prolactin deserves a spot on your suspect list.
What’s Causing Your Prolactin to Spike?
This is where the detective work begins. High prolactin doesn’t just happen randomly. There’s always a reason, though sometimes that reason takes effort to uncover.
Prolactinomas are the most common culprit—benign tumors on the pituitary gland that pump out excess prolactin. Before you panic, understand that “tumor” doesn’t automatically mean cancer. These are typically small, slow-growing, and highly treatable.
Medications are another major factor. Antipsychotics, antidepressants (particularly SSRIs), blood pressure medications, and even some anti-nausea drugs can elevate prolactin. If you’ve started a new medication and your fertility has tanked since then, connect those dots with your doctor.
Hypothyroidism creates an interesting twist. When thyroid hormone is low, your body compensates by producing more TRH (thyrotropin-releasing hormone), which inadvertently stimulates prolactin production. It’s hormonal collateral damage.
PCOS (polycystic ovary syndrome) sometimes coexists with high prolactin, though the relationship isn’t entirely straightforward. Hormonal imbalances often show physical symptoms; read more in Facial Hair & Acne: Early Hormonal Signs of Infertility.
Chronic stress can also push prolactin levels up. The same hormonal pathways that respond to stress can trigger prolactin release. It’s yet another reminder that your mental state and reproductive health are intimately connected.
The Telltale Signs You Shouldn’t Ignore
Some symptoms of high prolactin are obvious. Others are subtle enough that you might dismiss them as unrelated quirks.
The most distinctive sign? Galactorrhea—spontaneous milk production when you’re not pregnant or nursing. It might be just a few drops when you squeeze your nipple, or it could be more noticeable leaking. Either way, it’s your body waving a red flag.
Irregular or absent periods are another glaring indicator in women. If your cycle used to be clockwork and now it’s all over the place, prolactin might be the disruptor.
Headaches and vision problems can signal a larger prolactinoma pressing on nearby structures in your brain. This is less common but more urgent if present.
For men, gynecomastia (breast tissue enlargement) can develop, along with the sexual dysfunction mentioned earlier.
Here’s the tricky part: some people have elevated prolactin with zero symptoms. They only discover it when investigating infertility. That’s why testing is crucial if you’ve been trying to conceive without success.
Getting Diagnosed: It’s More Than Just One Blood Test
If your doctor suspects high prolactin, they’ll order a blood test. Simple enough, right? Not quite.
Prolactin levels fluctuate throughout the day and can spike temporarily due to stress, exercise, even a heavy meal. Having your blood drawn can itself cause a temporary rise—something called “stress-induced hyperprolactinemia.”
For an accurate reading, the test should ideally be done:
- In the morning, when levels are most stable
- After you’ve been sitting quietly for at least 30 minutes
- Ideally repeated if the first test shows elevation, to confirm it’s consistently high
A single mildly elevated result doesn’t necessarily mean you have a problem. Persistent elevation across multiple tests is what matters.
If prolactin is confirmed high, your doctor will likely order an MRI of your pituitary gland to check for tumors. They’ll also test your thyroid function, since hypothyroidism is such a common contributor.
Treatment: Yes, This Is Fixable
Here’s the good news that often gets buried beneath all the anxiety: hyperprolactinemia is one of the most treatable causes of infertility.
Dopamine agonists like cabergoline and bromocriptine are the frontline treatments. These medications work by mimicking dopamine, which naturally suppresses prolactin production. Most people see their prolactin levels normalize within weeks, and fertility often returns shortly after.
Cabergoline tends to be preferred because it’s taken less frequently (usually twice a week vs. daily) and has fewer side effects. Some people experience nausea or dizziness initially, but these typically subside.
If a prolactinoma is the cause, these medications don’t just lower prolactin—they often shrink the tumor itself. Surgery is rarely needed and reserved for cases where medications fail or tumors are large and causing significant problems.
Treating underlying causes is equally important. If hypothyroidism is contributing, thyroid hormone replacement can bring prolactin down naturally. If medication is the culprit, your doctor might switch you to an alternative that doesn’t affect prolactin.
For those seeking specialized care, consulting a fertility hospital in Chennai can provide comprehensive evaluation and treatment plans tailored to your specific hormonal profile.
The Fertility Comeback: What to Expect
Once treatment begins, the timeline to restored fertility varies. Some women ovulate again within a few weeks of starting medication. For others, it takes a few months for their cycles to regulate fully.
Men typically see improvements in sperm parameters within three months—the time it takes for new sperm to mature. Sexual function often rebounds more quickly as testosterone levels recover.
The key is patience and consistent monitoring. Your doctor will recheck your prolactin levels periodically to ensure they’re staying in normal range. Dosage adjustments are common in the first few months.
Many people worry about taking medication during conception attempts. Rest assured, cabergoline and bromocriptine are generally considered safe when trying to conceive, though your doctor will advise you on the best approach for your situation. Some practitioners prefer to stop the medication once pregnancy is confirmed, while others continue it through the first trimester, depending on individual circumstances.
When Prolactin Isn’t the Only Villain
Infertility is rarely a solo act. High prolactin might be part of a larger hormonal picture that includes thyroid issues, PCOS, or other endocrine imbalances.
This is why comprehensive fertility evaluation matters. Testing prolactin in isolation tells you something, but not everything. A thorough workup examines the full hormonal symphony—thyroid function, sex hormones, metabolic markers—to understand where things are breaking down.
Sometimes addressing prolactin alone solves the fertility puzzle. Other times, it’s one piece of a multi-pronged treatment approach.
The Bottom Line
High prolactin is one of those conditions that sounds intimidating but is actually quite manageable once identified. It hijacks your reproductive system through very specific mechanisms—suppressing GnRH, tanking your sex hormones, preventing ovulation or sperm production.
But here’s what matters most: it’s detectable with a simple blood test and treatable with medication that works remarkably well for most people.
If you’re struggling with infertility and experiencing any of the symptoms mentioned—irregular periods, galactorrhea, low libido, sexual dysfunction—push for prolactin testing. Don’t let it be the overlooked culprit that extends your fertility journey unnecessarily.
Your body isn’t broken. It’s just receiving the wrong signals. Once you correct the message, the reproductive machinery often fires back up beautifully. And that’s a comeback story worth pursuing.